


Speech And Language
Contents:
1.
What is Language and what is Speech
2.How
Speech Produce?
3.Speech and Language
Disorder
4.Specialists in
Speech-Language Therapy
5.When is Therapy
Needed?
6.Helping your Child
1.
What Is Language? What Is Speech?
Kelly's 4-year-old
son, Tommy, has speech and language problems. Friends and family have a hard
time understanding what he is saying. He speaks softly, and his sounds are not
clear.
Jane had a stroke. She
can only speak in one- to two-word sentences and cannot explain what she needs
and wants. She also has trouble following simple directions.
Language is different from speech.
Language is made up of socially shared rules that
include the following:
·
What words mean (e.g.,
"star" can refer to a bright object in the night sky or a celebrity)
·
How to make new words
(e.g., friend, friendly, unfriendly)
·
How to put words
together (e.g., "Peg walked to the new store" rather than "Peg
walk store new")
·
What word combinations
are best in what situations ("Would you mind moving your foot?" could
quickly change to "Get off my foot, please!" if the first request did
not produce results)
What
is Speech?
&
How Speech Produce?

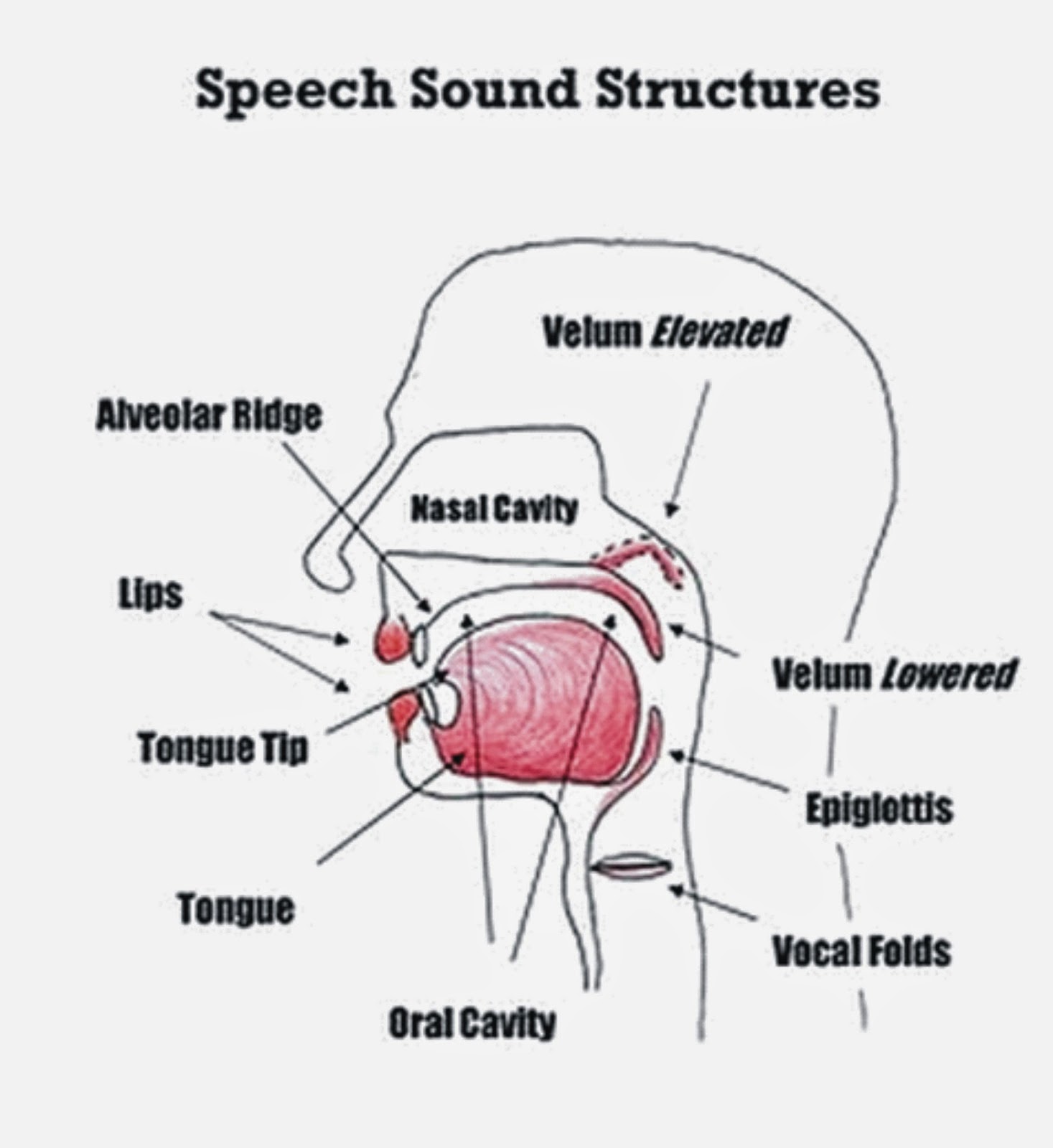
What is Speech? Speech is the physical production
of sound using our tongue, lips,
palate and respiratory system to
communicate ideas.
The Respiratory and Phonatory Systems

When we talk about the production of speech sounds it's best to start with the respiratory system. Speech is reliant on the powerful air flow that is supplied via our respiratory system.
What is Speech? Speech is the physical production
of sound using our tongue, lips,
palate and respiratory system to
communicate ideas.
The Respiratory and Phonatory Systems
When we talk about the production of speech sounds it's best to start with the respiratory system. Speech is reliant on the powerful air flow that is supplied via our respiratory system.
When we breathe out the air travels up from our lungs, through our windpipe and out through a structure in our throats called a voice box (larynx). The larynx shapes the sound of our voices. The sound, orphonation, is produced by a pair of vocal folds that are situated in the larnyx.
The voice box can change the nature of the sounds coming out of our lungs. When we turn the larynx on itvibrates. That is, the voice box works to make the quiet sounds coming out of our lungs into loud sounds.

The larynx can do this very fast. It can switch from quiet sounds to loud sounds and back again. The larynx does this without us even noticing it.
Articulation
Articulation is the name given to the precise movements of the tongue, palate, velum and lips to create the vowel and consonant sounds that make up the myriad phonemic elements of language. The amazing thing about articulation is that it must work in harmony with the respiratoryand phonatory systems. It does this amazingly well.
Articulation is the name given to the precise movements of the tongue, palate, velum and lips to create the vowel and consonant sounds that make up the myriad phonemic elements of language. The amazing thing about articulation is that it must work in harmony with the respiratoryand phonatory systems. It does this amazingly well.
What is
Speech? cont...
Once the air from our lungs reaches our mouth (oral cavity) we can then make speech sounds. We make speech sounds by using our tongue, teeth and lips to control the air as it passes through our mouth.
Our lips, tongue and teeth all work together to turn the air from our lungs into speech sounds, and, ultimately, spoken words. We have a name for the speech sounds made by the lips, tongue and teeth. These sounds are called consonants. Consonants are created by obstructions of the air flow created by our tongue, teeth, and lips. In contrast, vowels are generally produced with an open vocal tract.
Eliciting
Speech Sounds
Please click on the links to access information on how to elicit speech sounds for common speech sound errors.
Speech and Language Disorder
Please click on the links to access information on how to elicit speech sounds for common speech sound errors.
Speech and Language Disorder
·
Speech
·
Speech
is the verbal means of communicating. Speech consists of the following:
·
Articulation
·
·
Difficulties producing sounds
in syllables or saying words incorrectly to the point that listeners can't
understand what's being said.
·
How speech sounds are made (e.g., children must learn how to
produce the "r" sound in order to say "rabbit" instead of
"wabbit").
·
Voice
·
Use of the vocal folds and breathing to produce sound (e.g., the
voice can be abused from overuse or misuse and can lead to hoarseness or loss
of voice).
·
Fluency
problems such as stuttering, in which
the flow of speech is interrupted by abnormal stoppages, repetitions
(st-st-stuttering), or prolonging sounds and syllables (ssssstuttering).
·
The rhythm of speech (e.g., hesitations or stuttering can affect
fluency).
·
When
a person has trouble understanding others (receptive language),
or sharing thoughts, ideas, and feelings completely (expressive
language), then he or she has a language
disorder.
·
When
a person is unable to produce speech sounds correctly or fluently, or has
problems with his or her voice, then he or she has a speech disorder.
·
In
our example, Tommy has a speech
disorder that
makes him hard to understand. If his lips, tongue, and mouth are not moved at
the right time, then what he says will not sound right. Children who stutter, and people whose voices sound hoarse or nasal have speech
problems as well.
·
Jane
has a receptive and
expressive language disorder .
·
- Receptive
disorders: difficulties
understanding or processing language.
- Expressive
disorders: difficulty putting words
together, limited vocabulary,
- or
inability to use language in a socially appropriate way.
·
·
She
does not have a good understanding of the meaning of words and how and when to
use them. Because of this, she has trouble following directions and speaking in
long sentences. Many others, including adults with aphasia and children with learning disabilities, have language problems.
·
Language
and speech disorders can exist together or by themselves. The problem can be
mild or severe. In any case, a comprehensive evaluation by a speech-language pathologist (SLP) certified by the American
Speech-Language-Hearing Association (ASHA) is the first step to improving
language and speech problems.
·
If
you have concerns about a loved one's speech and/or language,
- Resonance
or voice disorders:
Problems with the pitch,
volume, or quality of the voice that distract listeners from what's being said.
These types of disorders may also cause pain or discomfort for a child when
speaking.
- Dysphagia/oral
feeding disorders:
These include
difficulties with drooling, eating, and swallowing.
Speech
Therapy
Specialists in Speech-Language Therapy
Speech-language pathologists (SLPs), often
informally known as speech therapists, are professionals educated in the study
of human communication, its development, and its disorders. They hold at least
a master's degree and state certification/licensure in the field, and a
certificate of clinical competency from the American Speech-Language-Hearing
Association (ASHA).
SLPs assess speech, language,
cognitive-communication, and oral/feeding/swallowing skills to identify types
of communication problems (articulation; fluency; voice; receptive and
expressive language disorders, etc.) and the best way to treat them.
Remediation
In speech-language therapy, an SLP will work
with a child one-on-one, in a small group, or directly in a classroom to
overcome difficulties involved with a specific disorder.
Therapists
use a variety of strategies, including:
·
Language
intervention activities:
The SLP will interact
with a child by playing and talking, using pictures, books, objects, or ongoing
events to stimulate language development. The therapist may also model correct
pronunciation and use repetition exercises to build speech and language skills.
·
Articulation
therapy:
Articulation, or sound
production, exercises involve having the therapist model correct sounds and
syllables for a child, often during play activities. The level of play is
age-appropriate and related to the child's specific needs. The SLP will
physically show the child how to make certain sounds, such as the "r"
sound, and may demonstrate how to move the tongue to produce specific sounds.
·
Oral-motor/feeding
and swallowing therapy:
The SLP will use a
variety of oral exercises — including facial massage and various tongue, lip,
and jaw exercises — to strengthen the muscles of the mouth. The SLP also may
work with different food textures and temperatures to increase a child's oral
awareness during eating and swallowing.
When Is Therapy Needed?
Kids might need speech-language therapy
for a variety of reasons, including:
·
hearing impairments
·
cognitive (intellectual, thinking) or other developmental delays
·
weak oral muscles
·
excessive drooling
·
chronic hoarseness
·
birth defects such as cleft lip or cleft palate
·
motor planning problems
·
respiratory problems (breathing disorders)
·
feeding and swallowing disorders
·
traumatic brain injury
Therapy should begin as soon as possible.
Children enrolled in therapy early (before they're 5 years old) tend to have
better outcomes than those who begin therapy later.
This does not mean that older kids can't
make progress in therapy; they may progress at a slower rate because they often
have learned patterns that need to be changed.
Finding a Therapist
It's important to make sure that the
speech-language therapist is certified by ASHA. That certification means the
SLP has at least a master's degree in the field and has passed a national
examination and successfully completed a supervised clinical fellowship.
Sometimes, speech assistants (who usually
have a 2-year associate's or 4-year bachelor's degree) may assist with
speech-language services under the supervision of ASHA-certified SLPs. Your
child's SLP should be licensed in your state and have experience working with
kids and your child's specific disorder.
You might find a specialist by asking your
child's doctor or teacher for a referral or by checking local directories
online or in your telephone book. State associations for speech-language
pathology and audiology also maintain listings of licensed and certified
therapists.
Helping Your Child
Speech-language experts agree that
parental involvement is crucial to the success of a child's progress in speech
or language therapy.
Parents are an extremely important part of
their child's therapy program and help determine whether it is a success. Kids
who complete the program quickest and with the longest-lasting results are
those whose parents have been involved.
Ask the therapist for suggestions on how
you can help your child. For instance, it's important to help your child do the
at-home stimulation activities that the SLP suggests to ensure continued
progress and carry-over of newly learned skills.
The process of overcoming a speech or
language disorder can take some time and effort, so it's important that all
family members be patient and understanding with the child.
Speech Sounds S. How to
Stimulate the /s/ Sound

Disclaimer: The techniques to be found on this page are written specifically for speech-language clinicians to use with their clientele.
Teachers and parents may also find useful advice here, but the information should not be considered as an alternative to comprehensive speech assessment and intervention. If your child has speech errors please ensure they are assessed by a qualified speech-language pathologist in your local area.
Unearthing
the Target Sound - Speech Sounds S cont..
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then produces a clear /s/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has produced.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this page.
The /s/ Sound - Speech Sounds S cont...
Correct /s/ Sound Production
The /s/ sound is a stream of air (fricative) sound. The /s/ is voiceless. That is, the larynx does not vibrate as it does on its voiced partner, the /z/ sound.
To produce a clear /s/ sound the tongue is raised high in the mouth to almost touch the alveolar ridge, the roof of the mouth. This action by the tongue should create a groove in the center of the tongue through which the air stream flows. Because the tongue constricts the space through which the breath stream travels, the /s/ sound should have a faint hissing quality to it.
Correct /s/ Sound Production
The /s/ sound is a stream of air (fricative) sound. The /s/ is voiceless. That is, the larynx does not vibrate as it does on its voiced partner, the /z/ sound.
To produce a clear /s/ sound the tongue is raised high in the mouth to almost touch the alveolar ridge, the roof of the mouth. This action by the tongue should create a groove in the center of the tongue through which the air stream flows. Because the tongue constricts the space through which the breath stream travels, the /s/ sound should have a faint hissing quality to it.
Some Common /s/ Sound Errors - Speech
Sounds S cont...
Lisp (Interdental) Sound Error - Speech Sounds S cont...
Perhaps the most common /s/ sound error is the interdental /s/. As the term suggests, the tongue pokes through (inter) the teeth (dental). The sound produced is actually the /th/ sound. So yes becomes yeth.
Demonstrate to the child what the error is by producing an interdental /s/ and comment on how the tongue pokes through the teeth and changes the sound to a /th/.
Next, demonstrate a correct /s/. Ask the child to feel with their tongue where the roof of their mouth is, particularly the alveolar ridge, the bumpy ridge just behind the top teeth. Have the child produce an air stream and note the position of their tongue. You can even block the air stream by touching the alveolar ridge with the tongue tip. This is an interesting sensation and immediately stops the air flow.
By lowering the tongue just a little, the air stream is released and a clear /s/ should issue forth. To ensure that the child doesn't poke their tongue tip through their teeth remind him/her that the tongue needs to be retracted (wound back) a little until it is just behind the teeth. It should never poke through the teeth.
Lateral /s/ Sound Error - Speech Sounds S cont
The lateral /s/ sound is made by the child directing the air stream to the sides (lateral) of the mouth (oral cavity). The sound produced has a 'slushy,' noisy quality to it.
The lateral /s/ is a difficult sound to eradicate. It requires the child to fundamentally alter the position of their tongue in the oral cavity. When producing a lateral /s/, the child will automatically retract the tongue and retract their lips much more than for a typical /s/ sound.
If you produce the lateral /s/ sound yourself you should notice that once the tongue is retracted the air stream slips over the sides of the tongue. Another feature is that the tongue blade and/or tip will touch the roof of the mouth. With a typical /s/ sound this never happens.
Because the air escapes around the sides of the tongue, there is a much larger space for the air to travel through, which, again, is much different from the typical /s/. This escaped air volume produces the slushy sound quality.
To effectively combat lateral /s/, the child needs to produce and develop a central air flow. That is, the air stream needs to flow along the central groove of the tongue, not escape around the sides.
One way of doing this is for the child to feel in their mouth for the location of the alveolar ridge. Ask the child to feel for the bumpy ridge just behind their top teeth at the roof of the mouth. Use the terms roof of mouth or top of mouth, depending on the child's ability to conceptualize their own oral cavity.
With their tongue tip touching the alveolar ridge, just behind the top teeth, ask the child to lightly pucker their lips. As in the instructions previous about the interdental /s/, the tongue position thus adopted will automatically block any outgoing air stream. And, importantly, this position automatically thrusts the tongue forward. Instruct the child to lower their tongue tip a fraction to release the airstream.
Due to the tongue position, the air stream cannot flow anywhere but over the top of the tongue, through the central groove. If this sequence is followed correctly a clear /s/ will occur.
Other segments devoted to Speech Sounds S will be added to as they become available.
Speech
Sounds sh. How to Elicit the sh Sound

Disclaimer: The techniques to be found on this page are written specifically for speech-language clinicians to use with their clientele.
Teachers and parents may also find useful advice here, but the information should not be considered as an alternative to comprehensive speech assessment and intervention. If your child has speech errors please ensure they are assessed by a qualified speech-language pathologist in your local area.
Producing
the Target Sound - Speech Sounds sh cont...
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then produces a clear /sh/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has modeled.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then produces a clear /sh/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has modeled.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this
page.
The /sh/ Sound - Speech Sounds sh
cont...
Correct /sh/ Sound Production
The /sh/ sound is a stream of air (fricative) sound. The /sh/ is voiceless. That is, the larynx does not vibrate as it does on its voiced partner, the /zh/ sound.
To produce a clear /sh/ sound the tongue is raised high in the mouth and pulled back so that the sides of the tongue contact the back teeth at the roof of the mouth. The lips are slightly protruded
The tongue's position creates a shallow groove in the center of the tongue over which the air stream flows. Due to the rear position of the tongue and the nature of the protruded lips the sound quality of the /sh/tends be louder than its other fricative (breath stream) cousins. This sound quality could be described to the child as loud and windy.
Some Common /sh/ Sound Errors - Speech
Sounds sh cont...
One of the more common sound substitutions is the /sh/ produced as a /s/. So, in connected speech, the sentence 'I bought some new shoes from the shop,' becomes 'I bought some new soes from the sop.
One of the more common sound substitutions is the /sh/ produced as a /s/. So, in connected speech, the sentence 'I bought some new shoes from the shop,' becomes 'I bought some new soes from the sop.
Eliciting the /sh/ Sound - Speech Sounds
sh cont...
Demonstrate to the child what a typical /sh/ sound looks like and sounds like. You do this by slightly protruding the lips and directing the breath stream over the middle of the tongue's blade. Elongate and exaggerate the /sh/ sound at this point.
Ask the child to feel with the sides of their tongue their upper back teeth. When the tongue is in the correct position, then have the child feel for the alveolar ridge with their tongue tip. The child then lowers their tongue slightly so that the tongue tip is roughly in the middle of the oral cavity, not touching any structures.
It's important at this point to remind the child to slightly pucker or protrude their lips. Try using a small mirror like a makeup mirror to give the child immediate feedback on how their lips need to be shaped.
Encourage the child to produce a loud, windy sound. Demonstrate the contrast between the /sh/ sound and the /s/ sound by alternating the sounds like this, /ssshhh/ 'loud and windy sound,' '/ssss/ thin and hissy sound.'
If the child is comfortably producing the /sh/ sound at this point have him/her produce the /sh/ - /s/ contrast. If the child is not yet sure about the new /sh/ sound then continue repeating the tongue and lips position, using the mirror to reinforce correct lip position.
It may take several sessions for the child to feel comfortable producing the /sh/ sound, or it may take only 5 minutes. That's the nature of speech therapy. Each child is different, of course, and each child learns new skills at different rates. An important consideration when teaching speech sounds is, how well does the child interpret oral instructions, and how well does the child visualize the relative position of their tongue in their mouth?
Some children struggle with the information overload and get a little mixed up when attempting to maintain correct tongue position at the same time as attempting correct lip position. This can be a little frustrating for both the child and the clinician. Patience and calm and lots of praise for the child's attempts are very important to encourage the child's confidence.
Speech
Sounds k. How to Elicit the /k/ Sound in Young Children

Disclaimer: The techniques to be found on this page are written specifically for speech-language clinicians to use with their clientele. Teachers and parents may also find useful advice here, but the information should not be considered as an alternative to comprehensive speech assessment and intervention. If your child has speech errors please ensure they are assessed by a qualified speech-language pathologist in your local area.
Unearthing
the Target Sound - Speech Sounds /k/ cont...
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then produces a clear /k/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has produced.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this page.
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then produces a clear /k/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has produced.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this page.
The /k/ Sound - Speech Sounds /k/
cont...
Correct /k/ Sound Production
The /k/ sound and its voiced partner the /g/ sound are what are known as velar plosives. Velar refers to the fact that the back of the tongue raises to contact the velum. This produces a brief blockage and a build up of pressure in the breath stream.
When the back of the tongue is lowered, there is a rapid, instantaneous burst of energy as the air pressure is released. Hence the reference to plosive. The intra-oral pressure build-up and release of the /k/ and /g/ sounds is truly explosive.
Common /k/ and /g/ Sound Errors - Speech
Sounds /k/ cont...
The most common /k/ sound error is the /k/ misarticulated as /t/. Similarly, the /g/ is misarticulated as /d/. This sound pattern is known as fronting. For instance, 'My new car,' becomes 'My new tar.' Again, the process also affects the /g/ sound. 'The goat got out the gate,' becomes 'The doat dot out the date.'
The /k/ to /t/ sound misarticulation is quite common. Fortunately, some children require only a few sessions of speech intervention before they quickly adopt the new /k/ and /g/ sounds, and even produce them spontaneously in words and connected speech.
For other children however the /k/ sound can be difficult to produce. In some situations it can take many sessions to produce an accurate /k/ sound.
The most common /k/ sound error is the /k/ misarticulated as /t/. Similarly, the /g/ is misarticulated as /d/. This sound pattern is known as fronting. For instance, 'My new car,' becomes 'My new tar.' Again, the process also affects the /g/ sound. 'The goat got out the gate,' becomes 'The doat dot out the date.'
The /k/ to /t/ sound misarticulation is quite common. Fortunately, some children require only a few sessions of speech intervention before they quickly adopt the new /k/ and /g/ sounds, and even produce them spontaneously in words and connected speech.
For other children however the /k/ sound can be difficult to produce. In some situations it can take many sessions to produce an accurate /k/ sound.
Eliciting the /k/ Sound - Speech Sounds
/k/ cont...
Demonstrate to the child what a typical /k/ looks and sounds like. You do this by opening your mouth slightly and lifting the tongue till it touches the velum at the back of the mouth. Mention that the tongue is pushed forward and down by the force of the air stream. Demonstrate this several times. Exaggerate the sound and repeating it in a sequence, such as /k /k//k/. You may choose to say , 'The /k/ sounds like a gun, /k/ /k/ /k/.
A clever way of stimulating the /k/ sound (Van Riper, 1963)is to ask the child to firmly place their tongue on his back lower teeth and position his hand in front of his mouth and feel the short bursts of air on his hand as he copies your correct /k/ model.
An important part of eliciting the /k/ sound is to enable the child to experience how different the /k/ sound is compared to the /t/ sound. The tongue position for the two sounds is radically different. The /t/ sound is made by the tongue thrusting forward in the oral cavity and the tongue tip touching the alveolar ridge. In contrast, the /k/ sound is made by the tongue pushing firmly to the back of the oral cavity which blocks the oral cavity off from the pharynx, until the tongue is lowered and the breath stream is released.
As clinicians, I don't think we fully appreciate how difficult it can be for some children to conceptualize the /k/ tongue position and how firmly it needs to be pushed against the velum. Children often report to me that the new /k/ sound 'feels weird' in their mouth.
Visual reference points can help some children conceptualize where their tongue is in their mouth.
Demonstrate to the child what a typical /k/ looks and sounds like. You do this by opening your mouth slightly and lifting the tongue till it touches the velum at the back of the mouth. Mention that the tongue is pushed forward and down by the force of the air stream. Demonstrate this several times. Exaggerate the sound and repeating it in a sequence, such as /k /k//k/. You may choose to say , 'The /k/ sounds like a gun, /k/ /k/ /k/.
A clever way of stimulating the /k/ sound (Van Riper, 1963)is to ask the child to firmly place their tongue on his back lower teeth and position his hand in front of his mouth and feel the short bursts of air on his hand as he copies your correct /k/ model.
An important part of eliciting the /k/ sound is to enable the child to experience how different the /k/ sound is compared to the /t/ sound. The tongue position for the two sounds is radically different. The /t/ sound is made by the tongue thrusting forward in the oral cavity and the tongue tip touching the alveolar ridge. In contrast, the /k/ sound is made by the tongue pushing firmly to the back of the oral cavity which blocks the oral cavity off from the pharynx, until the tongue is lowered and the breath stream is released.
As clinicians, I don't think we fully appreciate how difficult it can be for some children to conceptualize the /k/ tongue position and how firmly it needs to be pushed against the velum. Children often report to me that the new /k/ sound 'feels weird' in their mouth.
Visual reference points can help some children conceptualize where their tongue is in their mouth.
Speech
Sounds f. How to Elicit the /f/ Sound in Young Children.
Speech sounds f. This webpage gives practical advice on how to elicit the /f/ sound in young children.
Disclaimer: The techniques to be found on this page are written specifically for speech-language clinicians to use with their clientele.
Teachers and parents may also find useful advice here, but the information should not be considered as an alternative to comprehensive speech assessment and intervention. If your child has speech errors please ensure they are assessed by a qualified speech-language pathologist in your local area.
Eliciting
the Target Sound
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then models a clear /f/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has produced.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this page.
Imitation: Imitation is an important technique when teaching a child any new speech sound. Imitation requires the child to copy the clinician's correct model of a speech sound. For instance, the clinician first engages the child's full attention and then models a clear /f/ sound. The clinician is then silent and the child is encouraged to copy exactly the sound the clinician has produced.
In many cases of course the child will struggle to accurately reproduce the sound. This is fine, because the child's inability to correctly reproduce a clear target sound gives the clinician a good understanding of how the child's speech error is occurring.
Phonetic Placement: This is perhaps the most popular method of unearthing new and correct speech sounds in young children. Essentially the clinician demonstrates to the child how to correctly place their tongue, teeth and lips - their articulators, in order to produce the correct speech sound.
The techniques of imitation and phonetic placement will be explored on this page.
The /f/ Sound
Correct /f/ Sound Production

The /f/ sound is a stream of air (fricative) sound. The /f/ is voiceless. That is, the larynx does not vibrate as it does on its voiced partner, the /v/ sound.
To produce a clear /f/ sound the upper teeth lightly touch the lower lip. To an observer the impression is that the bottom lip is being bitten by the exposed upper teeth. However the upper teeth are merely touching the bottom, with only minimal pressure. When the breath stream flows through this constriction it produces the /f/ sound. Due to the constriction formed by the teeth and lips, the breath stream is forced forward and slightly down. The /f/ sound is unvoiced. Its partner, the /v/ sound, is voiced.
Common /f/ Sound Errors
A common sound substitution for the /f/ is the voiced /b/. So fish becomes bish.
Eliciting the /f/ Sound
Demonstrate to the child what a typical /f/ looks and sounds like. You do this by retracting the edges of your lips in the semblance of a slight smile. The upper teeth should be a little exposed and slightly touching the top of the bottom lip.
Blow the breath stream through the constriction created by the top teeth resting on the bottom lip. It's ok to exaggerate the sound level of the breath stream at this point to reinforce to the child that the /f/ is a stream of air (fricative) sound.
After demonstrating the correct position of the tongue and teeth, encourage the child to raise his bottom lip so that it is just slightly touching the upper teeth. It can be helpful to use a small mirror at this point to give the child a visual reference as to where his bottom lip needs to be positioned.
At this point instruct the child to blow air over his bottom lip. It can also be helpful for the child to position their finger in front of their lips to feel for the direction of the breath stream as it passes through the constriction created by the upper teeth and bottom lip.
When the child is able to find the lip position it is a good idea for them to change the position of the bottom lip to discover for them self the most comfortable position for producing a clear /f/ sound. The child does this by moving the bottom lip back and forth and noting the difference in breath stream constriction the movement of the bottom lip creates.
More about these visit this:
http://spl-education.blogspot.com




{kind=link}
3 Comments
Good work! Speech and language problems have become really popular nowadays. But sadly, there is very less attention paid to such issues in our society.
ReplyDeleteThanks for sharing this interesting post with us i found this helpful most effective receptive language disorder treatment in York Region, Toronto, Vaughan, Durham, Peel, North York & Markham. Contact us today!
ReplyDeleteThankyou for sharing such as nice article. Keep it sharing it will helpfull for me.
ReplyDeleteDown Syndrome Toronto